
[ad_1]
Study design and setting
This national web-based cohort study followed 17,640 participants over one year. Data are from the Joint Online Survey on COVID-19 and Work, a large-scale online cohort survey of Japanese workers registered in December 2020 during the “third wave” of COVID-19 infections. Extracted from the (CORoNaWork) project.20.Baseline survey and follow-up protocols are detailed20, 21, 22. Briefly, this study cohort included individuals who at baseline were workers between the ages of 20 and 65. They were selected through a systematic sampling strategy that considered factors such as gender, occupation, and region of residence in Japan. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Occupational and Medical Sciences (number R2-079). Informed consent was obtained.
From an initial recruitment pool of 33,087 participants, 6,051 participants with invalid responses were excluded, leaving 27,036 participants eligible for baseline analysis of the CORoNaWork project (Wave 1). Subsequently, in this cohort study, 18,560 participants responded to his 1-year follow-up survey in December 2021 (response rate, 68.6%, wave 2). Of these, 920 participants with his history of CHD at baseline were excluded (see profile in Supplementary Table S3), working 20-65 years old who at baseline had never experienced CHD. An analytic cohort of 17,640 individuals was obtained.
Primary outcome: development of CHD
The primary outcome was CHD development, which was confirmed retrospectively in the second wave. The question regarding CHD incidence in the second wave survey was worded as follows: “Are you currently receiving outpatient treatment or treatment for angina pectoris or myocardial infarction?” Participants were asked to choose one of the following options: Please answer: “I have never had this disease.” “I am currently receiving outpatient treatment or treatment.” “I previously received outpatient treatment or treatment, but I am currently receiving it at my own expense.” “I have been advised to undergo testing and treatment, but I have not visited a medical institution.” “I am currently cured or in remission (no longer requires treatment).”
The absence of CHD during the follow-up period was defined as the response “I have never had this disease.” Meanwhile, her other four responses indicated that he had developed CHD during the study period. The exact date of CHD onset was not available in this study.
occupational class
For occupational class, participants were grouped into upper-level non-manual workers (n = 1,886, 10.7%, consisting of managers and/or professionals) and others (n = 15,754, 89.3%). Ta.Go to previous research6,11. In general, with regard to socio-economic disparities in mortality rates, upper-level non-manual workers, including individuals from the highest occupational classes, Autonomy) tends to be the most advantageous.6,11.
Remote work and other covariates
Remote work is considered a key mediating variable that may influence changes in occupational CHD risk. A participant was classified as engaged in remote work if she reported working from home at least once a month during the baseline assessment.
The following basic confounding variables were considered when examining the association between occupational class and CHD risk: gender, age, and education (≥12 years). [high school] or 13 years [college or university]), household income (less than 2 million yen) [approximately 20,000 USD] or ¥2,000,000 or more). Furthermore, to further consider potential mediators, various covariates of behavioral factors (smoking, habitual drinking). [>â1 day/week]and physical activity [either aââ¥â30 min light sweating exercise more than once per week or aââ¥â1 h walking or equivalent activities more than once per week]), clinical factors (BMI, hypertension, diabetes), psychological distress (Kessler 6 score > 10), and long working hours (> 55 hours per week).twenty three.
statistical analysis
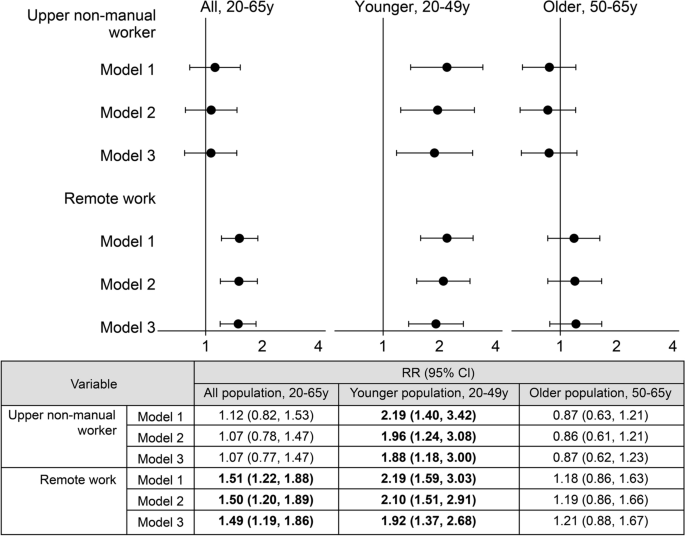
Risk ratios (RRs) and 95% confidence intervals (CIs) were estimated for CHD incidence among senior-level nonmanual workers. Other occupational groups served as reference groups. A two-level multilevel Poisson regression with robust variance was used, with the participant (level 1) nested within her 47 prefectures (level 2), and a random intercept for prefecture was applied.twenty four. Because this study lacked information on the precise timing of CHD onset, it was not possible to estimate incidence rate ratios. In the multivariate regression analysis, adjustments were made for the basic confounding variables of gender, age, education, and household income (Model 1). In Model 2, the key mediating variable of remote work was added. Finally, Model 3 considered all potential mediating variables. Furthermore, in Models 2 and 3, the estimated RR of remote work was accepted as an explanatory factor for his CHD incidence associated with remote work. For subgroup analyses, stratified analyzes were performed by age group: (i) younger age groups, 20–49 years, and (ii) older age groups, 50–65 years. Gender-specific analyzes were also performed.
Additionally, a causal mediation analysis using a four-way decomposition method (Figure 2) was conducted to estimate the proportion of occupational disparity in CHD risk for senior non-manual workers explained by remote work.twenty five. Exposure (senior-level non-manual worker), mediator (remote work), confounders (gender, age, education, household income), and outcome (CHD incidence) were defined.24, 25, 26, 27.Statistical significance was set at 0.05, and all P– Values were two-sided. Data were analyzed using STATA/MP17 (StataCorp LLC, College Station, TX, USA).
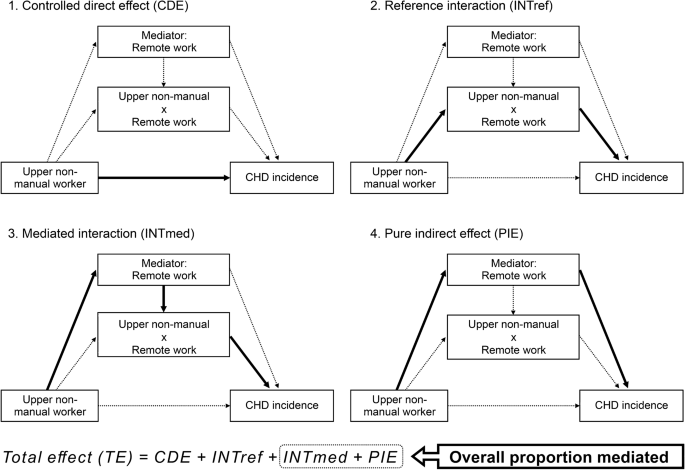
A four-way causal diagram of the association between senior-level non-manual employment, remote work, and incidence of coronary heart disease. Exposure (upper level non-manual workers), mediator (remote work), confounders (gender, age, education, household income), and outcome (coronary heart disease) [CHD] incidence) was defined. A four-way decomposition of the outcome (as a function of exposure, mediator, exposure-mediator interaction, and confounder) and mediator (as a function of exposure and confounder) was applied to the logistic regression model. The total effect (TE) of an exposure on an outcome in the presence of mediators with which it may interact is a four-component: fairness mediation (pure indirect effect, PIE), fairness interaction (reference interaction, INTref) It is broken down into ), both mediation and interaction (mediated interaction, INTmed), and neither mediation nor interaction (controlled direct effect, CDE): TE≠=CDE+INTref+INTmed’Euro+Pi. The overall proportion of the total effect explained by mediated effects (“sum of indirect effects”) was estimated using these four components as follows: (INTmed+PIE)/TE.
[ad_2]
Source link





