

[ad_1]
Study population
The 400 participants enrolled were classified according to oral glucose tolerance test (OGTT) values: 179 subjects with NGT, 137 with prediabetic isolated impaired fasting glucose and impaired glucose tolerance (IFG/ IGT), and 84 people were newly diagnosed with T2DM. The clinical characteristics of the subjects are reported in Table 1. At the time of enrollment, patients were not receiving any existing drug therapy. No statistically significant differences were observed between the three groups regarding age, gender, body mass index (BMI), smoking habits, systolic blood pressure (SBP), diastolic blood pressure (DBP), HDL and LDL cholesterol . In contrast, a significant increase in fasting plasma glucose (FPG) was observed (p< 0.0001), 2-hour plasma glucose (p< 0.0001), fasting plasma insulin (FPI) (p< 0.0001), 2-hour plasma insulin (p< 0.0001). Additionally, Matsuda/Index (p< 0.0001). Additionally, a significant increase in high-sensitivity C-reactive protein (hs-CRP) was observed (p< 0.0001), HbA1c (p< 0.0001), platelet count (PLT) (p= 0.003), triglycerides (TG) (p= 0.001) and decrease in estimated glomerular filtration rate (e-GFR) (p< 0.0001). Interestingly, MPV values gradually increased from the NGT group to the T2DM group (p< 0.0001) (Figure 1). Additionally, TyG scores significantly increased with worsening metabolic status (p< 0.0001) (Figure 1).
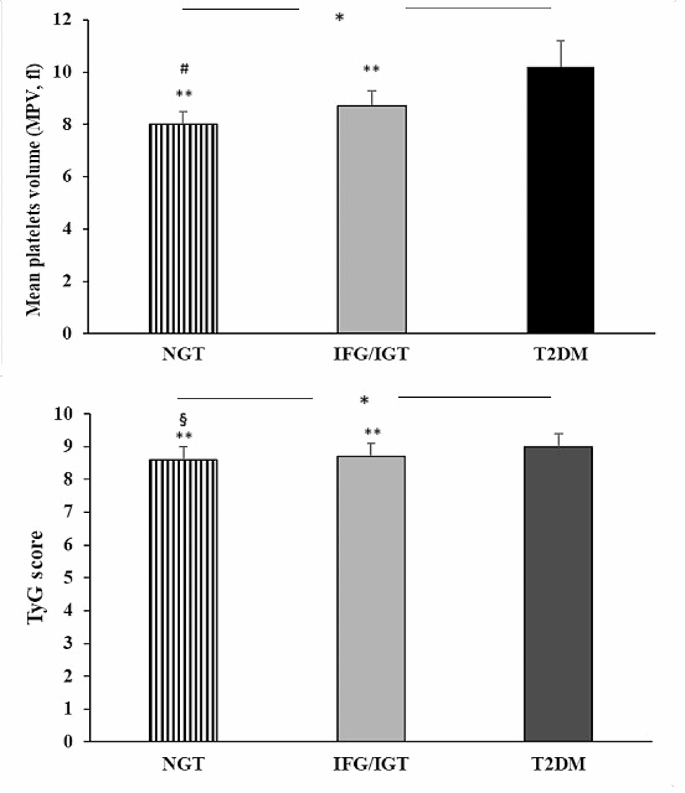
Graphical representation of MPV values and TyG scores detected in NGT, IGT/IFG, and T2DM patients. Data are mean ± standard deviation. *p< 0.0001 (ANOVA); § p= 0.007 IGT/IFG,** p< 0.0001 vs. DM2, # p< 0.0001 vs. IFG/IGT (Bonferroni post hoc test). NGT = normal glucose tolerance. IGT = impaired glucose tolerance. IFG = impaired fasting glucose T2DM = type 2 diabetes
From the Bonferroni post-hoc test, T2DM patients compared to NGT subjects had higher Matsuda/index (p< 0.0001) and the inflammatory profile indicated by hs-CRP (p< 0.0001), higher MPV value (p< 0.0001), increase in PLT count (p< 0.0001). Furthermore, prediabetic and T2DM patients showed higher MPV values (p< 0.0001) when compared to the NGT group. Furthermore, a significant difference in MPV values was observed when comparing the IGT/IFG group and the T2DM group (p< 0.0001). Regarding Tyg score, the NGT patient showed significantly lower values compared to her IGT/IFG (p= 0.007) and T2DM patients (p< 0.0001), furthermore, prediabetic patients showed lower Tyg score values when compared to the T2DM group (p< 0.0001).
Evaluation of arteriosclerosis and echocardiographic parameters
Peripheral and central hemodynamic parameters are reported in Table 2. We found some differences in the atherosclerosis parameters of the three study groups. As expected, a significant increase in PWV was observed (p< 0.0001), increase index (AI%) (p< 0.0001), increased pressure (AP) (p< 0.0001), central systolic blood pressure (c-SBP) (p< 0.0001) and central pulse pressure (c-PP) (p< 0.0001), demonstrating an increase in arterial stiffness with deterioration of metabolic status. Bonferroni post hoc tests showed higher AI% values for T2DM and IGT/IFG subjects (p< 0.0001) and AP (p< 0.0001), compared with the NGT group.
Table 3 shows the morphological and functional echocardiographic parameters of the entire population and the three study groups. There was a significant increase in left ventricular mass (LVM) as we progressed from the first group to the third group (p< 0.0001), left ventricular mass index (LVMI) (p< 0.0001), left ventricular diastolic diameter (LVDD) (p< 0.0001), diastolic posterior wall (dPW) (p< 0.0001). No statistically significant differences were detected between the three groups regarding left global systolic function assessed as ejection fraction (EF). In contrast, from the first group to his third group, there was a progressive decline in myocardial deformation and left global systolic function assessed as global longitudinal strain (GLS) (p< 0.0001). In particular, T2DM and prediabetic patients had more impaired GLS compared to NGT subjects (p< 0.0001).
Regarding the index of right global systolic function, a significant decrease in TAPSE values was observed (p< 0.0001), accompanied by deterioration of metabolic status. Regarding diastolic function, the E/A ratio was significantly lower in the T2DM group (p< 0.0001).
Compared with the left atrial volume index (LAVI) parameter, it gradually increased from healthy subjects to T2DM patients (p= 0.001).
linear regression analysis
Linear regression analysis was performed between MPV, GLS, and PWV considered as dependent variables and various covariates (Table 4).
MPV was significantly and directly correlated with HbA1c (r= 0.251, p< 0.0001), hs-CRP (r= 0.120, p= 0.009), PLT (r= 0.187, p< 0.0001), TyG score (p= 0.273, p< 0.0001), BMI (r= -0.165, p= 0.001) and age (r= 0.107, p= 0.018), and the Matsuda index (r= -0.446, p= < 0.0001) and e-GFR (r= -0.399, p< 0.0001).
Thereafter, GLS was significantly and directly correlated with E/e’ (r= 0.409, p= < 0.0001), LVMI (r= 0.329, p= < 0.0001), MPV (r= 0.383, p< 0.0001), Hs-CRP (r= 0.100, p= 0.038), SBP (r= 0.159, p= 0.001), DBP (r= 0.126, p= 0.006) and TyG score (r= 0.177, p< 0.0001), Matsuda index (r= -0.299, p< 0.0001) and e-GFR (r= -0.112, p= 0.014).
When PWV was considered as the dependent variable, the results showed a significant and direct correlation with MPV (r= 0.451, p< 0.0001), hs-CRP (r= 0.111, p= 0.015), LDL cholesterol (r= 0.109, p= 0.016) and TyG score (r= 0.111, p= 0.026), and the Matsuda index (r= -0.382, p< 0.0001), e-GFR (r= -0.152, p= 0.001) and HDL cholesterol (r= -0.140, p= 0.003).
Variables that reached statistical significance were introduced into a stepwise multivariate linear regression model to identify independent predictors of MPV, PWV, and GLS (Table 5).
In the entire study population, the Matsuda index was the main predictor of MPV, accounting for 19.7% of its variation. e-GFR, HbA1c, and PLT added an additional 7.7%, 1.7%, and 1.1%, respectively. Moreover, E/è was the main predictor of GLS, justifying 16.5% of its variation. MPV was his second predictor explaining 8.3% of the variation, and LVMI added another 2.0%. Considering PWV, MPV was the main predictor explaining 20.1% of its variation, while Matsuda index and LDL added 3.5% and 1.2%, respectively.
ROC curve analysis
To further clarify the diagnostic value of MPV for atherosclerosis and subclinical myocardial injury, we performed receiver operating characteristic (ROC) curve analysis. We used his PWV as the gold standard for atherosclerosis. The considered cutoff was 10 m/s. GLS was the gold standard for determining the severity of subclinical myocardial injury. The considered cutoff was – 17%. ROC curve analysis showed that the area under the curve (AUC) values for MPV for PWV and GLS were 0.76 (standard error 0.030, 95% CI 0.70 to 0.82, respectively). p< 0.0001) and 0.64 (standard error 0.033, 95% CI 0.57 to 0.70, p< 0.0001) (Figure 2).
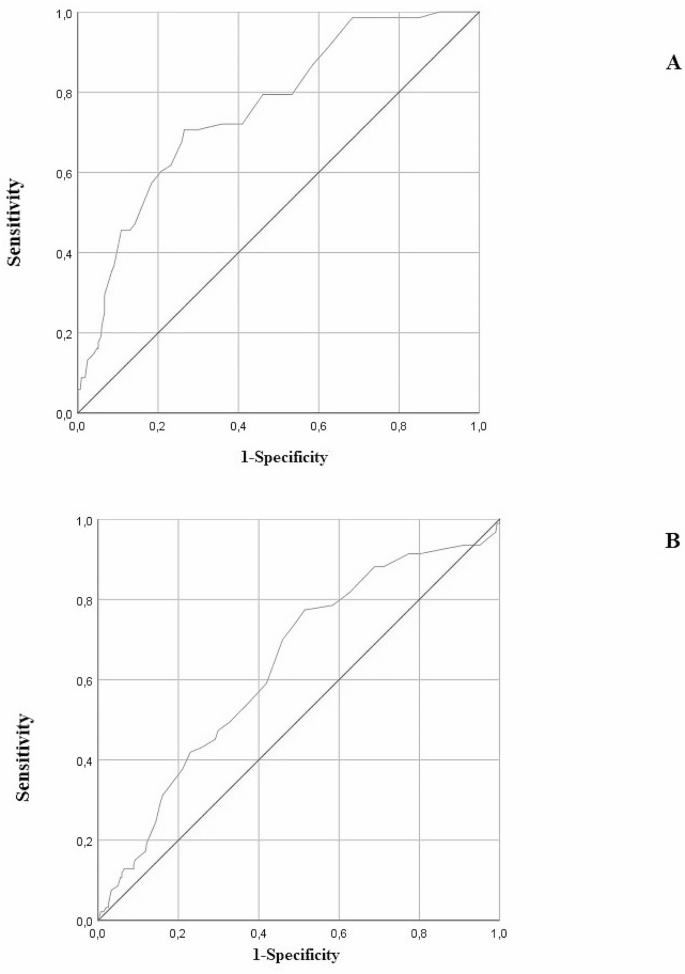
Analysis of ROC curves to determine MPV stratified according to PWV (a) and GLS (B)
[ad_2]
Source link





