
[ad_1]
March 14, 2024
2 minute read
Important points:
- Patients with lupus and gout had more than twice the risk of several cardiovascular diseases.
- The researchers said rheumatic diseases should be considered an “independent risk factor” for cardiovascular disease.
Among patients with rheumatic diseases, the risk of cardiovascular complications is highest during the period immediately preceding or following initial diagnosis, according to data published in . Arthritis and Rheumatism Seminar.
“Selected traditional [cardiovascular (CV)] Although risk factors may be more prevalent among certain rheumatic diseases, the increased risk of cardiovascular comorbidities cannot be fully explained by traditional cardiovascular risk factors. ” hannah kaisa Aaramar, and colleagues from Tampere University Hospital in Finland write: “Research shows that the risks of certain cardiovascular diseases are: [rheumatoid arthritis] and [systemic lupus erythematosus] It has been increasing since before diagnosis. However, most studies do not provide information about the temporal relationship between the onset of cardiovascular disease comorbidities and the diagnosis of rheumatic diseases. ”

To determine the risk of cardiovascular complications in rheumatology patients and when they are likely to occur, Aaramaa et al. analyzed data from FinnGen, Finland’s national medical registry. These included records of her 321,302 patients diagnosed with rheumatism or cardiovascular disease from January 2000 to December 2014. Each case of rheumatic disease was matched with her 20 randomly selected controls. The researchers used logistic regression, adjusting for age and sex, to calculate odds ratios for cardiovascular disease.
Rheumatic diseases included in the cohort were seropositive and seronegative RA, ankylosing spondyloarthritis, psoriatic arthritis, primary Sjogren’s syndrome, SLE, and gout. Meanwhile, cardiovascular comorbidities of interest were major coronary heart disease events, chronic heart failure, atrial fibrillation or flutter, valvular heart disease, venous thromboembolism, and ischemic stroke.
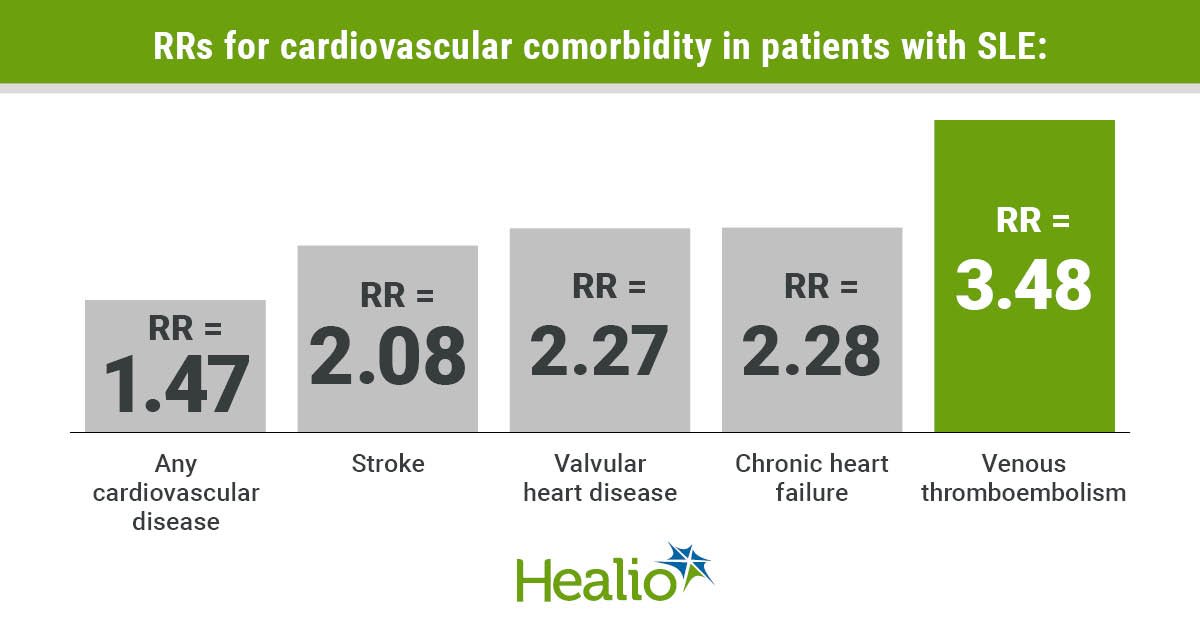
According to the researchers, the RR for cardiovascular complications ranged from 1.14 (95% CI, 1.02 to 1.26) for patients with PsA and 2.05 (95% CI, 1.67 to 2.52) for patients with SLE. Patients with SLE and gout have been shown to have more than twice the risk of chronic heart failure, valvular heart disease, and venous thromboembolism, while SLE is also associated with a relative risk of stroke of 2.08 (95% CI, 1.2-3.61) Was.
Meanwhile, the researchers found that the risk of cardiovascular complications before and after diagnosis of rheumatic diseases was “quite similar” overall, but after diagnosis of RA, PsA, primary Sjögren’s syndrome, and SLE. It was the highest in less than a year. The OR for cardiovascular disease in gout patients was “clearly elevated” 10 years before and 1 year after gout diagnosis, the researchers wrote. The OR for cardiovascular comorbidities was highest within 5 years of AS diagnosis.
“Our results highlight the increased risk of cardiovascular comorbidity across all rheumatic diseases very early in the disease course, making rheumatic disease independent of cardiovascular disease. “We encourage consideration of this risk factor as a risk factor,” Aramaa et al. “We also need to pay attention to the following rising risks. [venous thromboembolism] For all patients with rheumatic diseases. ”
Information source/disclosure information
collapse
Disclosure: Aaramaa reports speaking fees from Novartis and conference travel support from UCB Pharma and Medac. Please refer to this study for relevant financial disclosures of all other authors.
[ad_2]
Source link





